
Inside a Dementia Care Plan | Example
Ready to talk about it?

A quick note before jumping in
We made a deliberate choice when building this website.
Most homecare websites tell you very little. There is a list of services, a phone number, and some reassuring language about dignity and compassion. What actually happens during a visit, how carers are trained, what a care plan looks like, what we cannot do and who can — none of that is there. You are expected to call, be reassured, and trust that the details will work out.
We do not think that is good enough. Not for a decision this important.
So we have tried to write this website for the person who wants to understand properly — the adult child lying awake at 2am with questions they have not yet found answers to, the family navigating a dementia diagnosis for the first time, the person who simply wants to know what they are actually agreeing to before they pick up the phone.
Every service page explains not just what we offer but how it works, what it involves, and where our role ends and someone else's begins. The FAQ answers the questions people actually ask, including the uncomfortable ones. The blog covers the topics that affect the people we look after — in detail, with honesty, and with the specific knowledge of a team that has been doing this work in North Shropshire for fourteen years.
You do not need to read any of it. You are welcome to simply call us, tell us your situation, and let us guide you through the rest. That is exactly what most families do, and it works perfectly well.
But if you want to read — if you want to understand the medication protocols before you commit, or see what a real care plan looks like, or know how we approach a difficult dementia morning — it is all here. Because we think the families who trust us deserve to know exactly what that trust is built on.
We want to be more open about our work than anyone else in this sector. This website and resources like this page is our attempt to do that.
The Example
One of the questions we are asked most often by families considering homecare for the first time is: what does a care plan actually look like?
The honest answer is that a good care plan looks nothing like a medical form. It is not a list of tasks. It is a detailed, living document about a specific person — who they are, what they need, how they prefer to receive it, and what matters most to them. It is the instruction manual that every carer reads before their first visit, and returns to every time something changes.
To show you what we mean, we have created a detailed example care plan for a fictional client — Emily — based closely on the kind of plans we develop with our real clients and their families across North Shropshire. All details are invented, but the format, the level of detail, and the clinical content are representative of how we actually work.
If you are arranging care for a relative with dementia and wondering what the process involves, this is it.
NORTH SHROPSHIRE HOMECARE
Individual Care Plan
Document reference: NSHC/CP/EXAMPLE Date of plan: June 2026 Review date: September 2026 Completed by: Alice Allen, Registered Manager Status: Example document — for illustrative purposes only
Section 1 — About Emily
Full name Emily Margaret Whitmore
Preferred name Emily — never "Em"
Date of birth 14 March 1948 (age 78)
Sexuality Straight
Address A rural bungalow, outskirts of Prees, North Shropshire
Lives with Alone. Widowed 2019.
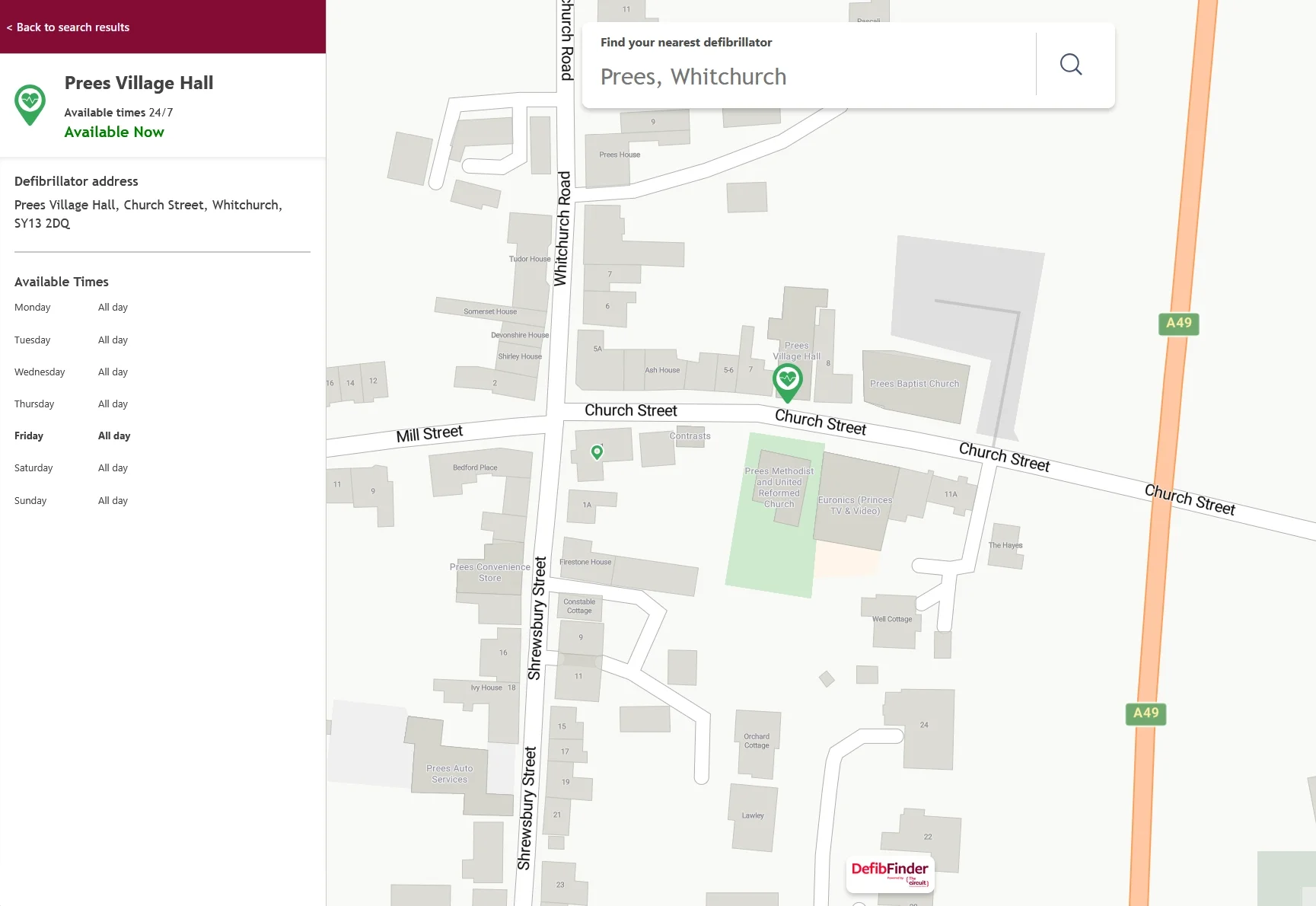
Property type Single-storey bungalow, no steps, walk-in shower, downstairs WC. Key safe fitted at front door — code held by NSHC office.
Nearest Defibrillator Prees Village Hall (24/7) code:8795.
About Emily — written with her family:
Emily was a primary school teacher at a village school outside Wem for over thirty years. She retired in 2010. She is the mother of two adult children — James (lives in Shrewsbury) and Catherine (lives in Manchester). She has four grandchildren whom she adores.
Emily was an avid gardener — her back garden is her great pride and she becomes visibly distressed if it appears neglected. She baked every Friday without fail for most of her adult life and still responds warmly to the smell of bread or cake. She was a member of Whitchurch Choral Society for twenty years and music — particularly hymns and 1960s popular music — has a noticeably calming effect on her.
Emily has always valued her independence fiercely and finds it difficult to accept help with tasks she once did easily. She is a private person and dislikes feeling observed or managed. She responds best to being asked rather than told, and to being given choices rather than instructions.
Emily's faith is important to her. She attended St Alkmund's Church in Whitchurch regularly before her mobility became more limited.
Why this section matters to families: This is the most important section of the entire care plan, and the one most care plans get wrong. A carer who knows Emily was a teacher, that her garden matters to her, that she finds hymns calming — that carer is not interchangeable with a carer who doesn't know any of this. The "About Me" section is what turns a generic visit into a meaningful one. We write this section with the family, not from a form.
Section 2 — Emergency Contacts
Name Relationship Phone Notes James Whitmore Son (next of kin) 07XXX XXXXXX First contact for all non-emergency matters. Works office hours Mon–Fri.
Catherine Patel Daughter 07XXX XXXXXX Second contact. Available most evenings. Prefers WhatsApp messages during working hours.
Dr S. Okonkwo GP 01948 XXXXXX Whitchurch Medical Practice. Emily has been with this practice for 20 years.
District Nursing Team NHS 01948 XXXXXX Contact for any wound care, catheter concerns, or clinical queries.
Severn Hospice (advice line) Palliative support 01743 236565 Not currently involved but number held for future reference.
In an emergency: Call 999 first. Then call James. Then call the NSHC office on 01948 411222 (answered 24 hours).
Do Not Resuscitate status: Emily holds an Advance Decision document, held on file at NSHC, with her GP, and displayed on the inside of the kitchen cupboard above the kettle. All carers have been made aware of its existence and location.
Why this section matters to families: The DNR/Advance Decision note is one families sometimes feel uncomfortable raising with a care provider. We raise it ourselves, because a carer arriving in an emergency needs to know where to find this document immediately. We hold a copy, we know where the original is, and we never put a carer in a position of not knowing what Emily's wishes are.
Section 3 — Diagnoses and Medical History
Condition Diagnosed Notes Alzheimer's disease (moderate stage) 2022 Diagnosed at memory clinic, Royal Shrewsbury Hospital. Currently under Dr Fiona Marsh, Consultant Geriatrician. Annual review.
Hypertension 2015 Managed with medication. Stable. Osteoarthritis (bilateral knees) 2018 Affects mobility, particularly on stairs and rising from low chairs.
Type 2 diabetes (diet-controlled) 2020 No insulin. Managed through meal timing and carbohydrate awareness. Review with practice nurse every 6 months. Hearing loss (bilateral, mild-moderate) 2019 Wears hearing aids in both ears. Right and left aids charge on bathroom shelf.
Recurrent UTIs Ongoing History of UTIs presenting as sudden confusion rather than typical urinary symptoms.
Any unexplained increase in confusion should prompt a GP contact within 24 hours.
Why this section matters to families: The UTI note is critically important and is a good example of why medical history in a care plan is not just background information — it is operational guidance. Emily's UTIs present as sudden confusion rather than the symptoms most people associate with a urinary infection. A carer without this information might attribute increased confusion to her Alzheimer's progressing and do nothing. A carer with this information knows to flag it immediately to the family and GP. That difference can mean days less suffering and the prevention of a hospital admission.
Section 4 — Current Medication
Medication Dose When Route Notes Donepezil (Aricept) 10mg Nightly, with evening drink Oral tablet Dementia medication. Must be taken consistently. Amlodipine 5mg Morning, with breakfast Oral tablet Blood pressure. Do not omit. Paracetamol 500mg x2 Twice daily (morning and evening) Oral tablet For arthritis pain. PRN — offer it, do not insist. Vitamin D 800IU Morning Oral capsule Prescribed by GP.
Medication administration level: Assisted administration. Emily cannot reliably manage her own medication. Carers prepare and offer medication, confirm it has been swallowed, and record on eMAR.
Known issues: Emily occasionally refuses her evening Donepezil if she is tired or unsettled. If she refuses, document it, do not force it, and notify the office if this happens on two or more consecutive evenings.
Allergies: Penicillin (documented reaction — rash and swelling, 1987). Allergy alert displayed on medication folder and on the kitchen noticeboard.
Why this section matters to families: The allergy alert is something families sometimes assume "the system" will handle. In a well-run care package it does — it is in the care plan, it is in the medication folder, it is on the noticeboard, and every carer is told verbally at handover. If Emily were ever admitted to hospital from home, the first thing the care coordinator would tell the ambulance crew is the penicillin allergy. This redundancy is deliberate. One note in one place is not enough.
Section 5 — Cognitive and Communication Profile
Current cognitive presentation (June 2026):
Emily is at a moderate stage of Alzheimer's. Her short-term memory is significantly impaired — she will typically not recall a visit that occurred the day before, and may ask the same question several times within a single visit. Her long-term memory is considerably better preserved; she speaks fluently and with pleasure about her teaching career, her late husband Robert, and her grandchildren's earlier childhoods.
Emily has periods of good clarity, typically in the morning after a settled night, and periods of significant confusion, most commonly in the late afternoon and early evening. The difference between a good morning and a difficult late afternoon can be considerable.
Communication guidance for carers:
Always introduce yourself by name at the beginning of every visit, even if you have visited Emily many times. Do not assume she remembers you.
Use her name frequently in conversation — it grounds her.
Speak clearly and at a slightly slower pace than normal. Do not raise your voice — Emily is not hard of hearing when her aids are in.
Ask one question at a time. Do not offer more than two options in a choice.
If Emily becomes distressed or confused, do not argue or correct. Redirect gently — toward a familiar topic, a familiar object, or a familiar activity.
If Emily refers to Robert in the present tense, do not correct her. Follow her lead. Correcting her that Robert has died causes acute distress and serves no purpose.
The phrase "Let's have a cup of tea" is reliably effective at resetting a difficult moment.
Orientation aids in the home:
A large-print whiteboard in the kitchen displays: today's date, day of the week, the carer's name for that visit, and a brief note of what is happening that day. Carers update this board at the start of every visit.
A printed photograph board in the sitting room shows labelled photos of family members, updated by James in April 2026.
Why this section matters to families: The instruction not to correct Emily about Robert being alive is one that families sometimes find difficult to process — it can feel like colluding in a confusion. Our experience, and the evidence from dementia care research, is consistent: orienting a person with dementia to a painful reality they cannot retain causes repeated grief without any therapeutic benefit. Emily cannot hold the information. What she can hold is the feeling that a visit caused her distress. We protect her from that.
Section 6 — Daily Routine
Morning Visit — 8:00am (approximately)
Task Detail Greeting and orientation Introduce yourself. Update whiteboard. Check Emily's general presentation — mood, mobility, any visible signs of a difficult night. Hearing aids Check both aids are in and functioning. If not on, assist Emily to insert them before conversation continues. Personal care Emily prefers a shower on Monday, Wednesday, and Friday.
On other days, a wash at the bathroom sink is sufficient. She is modest and prefers a female carer for personal care — this has been accommodated in the rota. Allow Emily to do as much as she is willing and able to do independently. Prompt before assisting. Dressing Emily's clothes for the day are laid out the previous evening by the late carer. Allow Emily to choose between two options if she wishes. She has strong preferences about colour — she dislikes brown and will often refuse to wear it.
Breakfast Emily's preference: two slices of white toast with butter and marmalade, a glass of orange juice, and one cup of tea (strong, small amount of milk, no sugar). Diabetes: avoid sugary cereals or fruit juice in large quantities. Ensure she eats before morning medication. Medication After breakfast — see Section 4. Record on eMAR. Garden check If weather permits and Emily is well-oriented, 10–15 minutes in the garden is highly beneficial. She does not need to do anything — simply being in the garden improves her mood markedly. If she wants to do light deadheading or potting, facilitate this carefully. Handover note Complete the visit record before leaving. Note mood, appetite, any concerns, whether medication was taken.
Lunchtime Visit — 12:30pm (approximately)
Task Detail Meal preparation Hot meal preferred at lunchtime — Emily eats better at lunch than in the evening. Refer to the weekly meal planner on the fridge (updated by James on Sundays). Emily likes traditional food: soup, sandwiches, jacket potatoes, light pasta. She dislikes spicy food. Hydration Emily does not drink enough fluid independently.
Offer a full glass of water or diluted squash on arrival and again with the meal. Target: at least 4 glasses of fluid across the day. Companionship The lunchtime visit should not feel like a task completion exercise. Sit with Emily while she eats. Talk. Ask about her grandchildren, her garden, her memories of teaching. The quality of this visit matters as much as the food. Afternoon orientation If Emily appears confused about the time of day, gently reorient using the whiteboard. Do not argue — redirect.
Evening Visit — 5:30pm (approximately)
Emily frequently becomes more confused, more anxious, and occasionally more resistant to care in the late afternoon. Approach this visit with extra patience. Do not rush. Evening meal Light meal — Emily's appetite is lower in the evening. Soup, beans on toast, scrambled eggs are all acceptable and well-received. Ensure she has eaten something. Medication Donepezil 10mg with evening drink — see Section 4. If declined, document and notify office if repeated. Preparation for night Lay tomorrow's clothing options on the chair. Ensure heating is set correctly (Emily is often cold — thermostat should be no lower than 19°C overnight). Check back door is locked. Ensure a glass of water and a biscuit are within easy reach of the bed. Night light The hallway night light should be on before leaving. Emily has been found confused in darkness on two occasions — the light significantly reduces night disorientation. Final handover note Complete visit record. appetite, medication, any concerns.
Why this section matters to families: Families often ask whether carers really follow the routine or whether it is just written down. The honest answer is that a well-written routine, built around the individual's actual preferences and patterns, is followed because it works. Emily eating better at lunch than in the evening is not a preference to note and ignore — it is a clinical fact that shapes what we offer and when.
Section 7 — Mobility and Moving & Handling
Current mobility status: Emily is independently mobile on flat surfaces. She uses a walking stick, kept by the front door, for outdoor walking and longer indoor distances. She is unsteady on rising from low chairs — the sitting room sofa is too low for her and she should be directed to the upright armchair by the window when possible.
Fall history: One fall recorded February 2026 — tripped on a rug in the hallway. Rug has been removed. No injury sustained. Incident reported to GP and family.
Moving and handling assessment: No hoist or transfer equipment currently required. Standard assist technique for rising from chair if needed — two-point contact, verbal guidance, allow Emily to lead the movement.
Footwear: Emily must wear her slippers or shoes at all times when mobile indoors — not socks alone. Her slippers are kept by the bedroom door. This is a falls risk management requirement.
Why this section matters to families: The rug removal is a good example of how care plans respond to incidents rather than simply recording them. A fall happened, the cause was identified, and the environment was changed. The care plan records this so that every subsequent carer — including any cover carer who has never visited before — knows the rug is gone and why, and knows Emily's specific fall risk profile.
Section 8 — Risk Assessments
Risk Level Management Falls Medium See Section 7. Night light in hallway. Upright chair preferred. Footwear protocol. Wandering Low-medium Emily has not wandered outside unsupervised but has been found at the front door in the evening on two occasions. Front door key is kept on a high hook she cannot easily reach. Carers check door is locked on every exit. Family have been consulted and are aware. Medication non-compliance Medium See Section 4. eMAR recording. Family notification protocol for repeated refusal. Nutrition and dehydration Medium See Section 6. Hydration target noted. Diabetes monitoring through meal content. Safeguarding Low No current concerns. Emily is at standard safeguarding awareness level. Any concerns to be reported immediately to Alice Allen and to Shropshire Adult Safeguarding on 0345 678 9044. Infection / UTI Medium See Section 3. Any unexplained confusion increase to trigger GP contact within 24 hours. Carer stress (family) Medium James visits weekly. Catherine visits monthly. Both have been offered information about respite care and Shropshire Carers. James has been provided with the Carers UK helpline.
Why this section matters to families: The inclusion of family carer stress as a formal risk in Emily's care plan is something that surprises many families. We include it because it is real, because it is common, and because carer burnout is one of the most predictable causes of a care package breaking down. We monitor it proactively rather than waiting for a crisis.
Section 9 — What a Good Day Looks Like / What a Difficult Day Looks Like
A good day: Emily is up and dressed before the carer arrives, or gets up quickly with minimal prompting. She is oriented to the morning, engages in conversation, asks about the carer's family. She eats well at breakfast and lunch. She spends time in the garden. She mentions Robert in the past tense. She laughs.
A difficult day: Emily is in bed when the carer arrives and resists getting up. She is confused about where she is or who the carer is. She asks repeatedly for Robert or for her mother. She eats little. She becomes tearful or agitated in the late afternoon. She goes to the front door in the evening.
What to do on a difficult day: Do not rush. Do not argue. Do not try to reorient through information — reorient through familiarity. Put the radio on (Classic FM or Radio 2 — she knows the songs). Make tea. Sit with her. If she is distressed beyond what gentle redirection can manage, call the office. Do not leave Emily alone when she is acutely distressed.
Document the difficult day fully. If difficult days are clustering — three or more in a week — notify Alice and James. This pattern can indicate a UTI, a medication change, a change in the progression of the condition, or an environmental factor. It requires clinical attention.
Why this section matters to families: Most care plans describe what to do. This section describes what to expect — and that is often more valuable. A carer who walks into a difficult day and has no frame of reference for it is a carer who might panic, rush, or inadvertently make things worse. A carer who has read this section knows that a difficult day has a shape, and knows what a good response looks like.
Section 10 — Review and Signature
This care plan will be reviewed: September 2026, or sooner if Emily's condition changes significantly, if an incident occurs, or if the family requests a review.
Reviewed and agreed by: Alice Allen, Registered Manager, North Shropshire Homecare ............... Date: .......... James Whitmore, next of kin ............... Date: ..........
Emily has been involved in the care planning process to the extent her capacity allows. Her preferences as expressed during the assessment have been incorporated throughout. A copy of this plan is held by NSHC, shared with James and Catherine, and a summary version is kept in the care folder in Emily's kitchen.
A Note to Families Reading This
If you are arranging care for someone living with dementia and this document feels more detailed than you expected — that is the point.
Every section of Emily's plan exists because it reflects something specific about Emily. The bread-baking memory. The garden. Robert. The UTI risk. The nearest defib. The penicillin allergy above the kettle. These details are not decoration. They are the difference between a carer who is providing care and a carer who is caring for Emily.
When we carry out a home assessment, this is what we are building toward. Not a form to file — a document that every person who enters Emily's home reads, understands, and works from.
If you would like to talk through what a care plan for your relative might involve, call us on 01948 411222 or email mail@nshomecare.co.uk. The assessment is free, and the conversation costs nothing.
North Shropshire Homecare The Coach House, 15/17 Green End, Whitchurch, SY13 1AD

Testimonials.
Discover why we are regarded as the "Gold Standard" for homecare in North Shropshire through the honest, unfiltered eyes of our clients and their loved ones. To provide you with total peace of mind, we also feature independent insights from our latest CQC (Care Quality Commission) inspection. These combined voices offer a complete picture of our commitment to safety, dignity, and clinical excellence. We are incredibly proud to share the feedback that not only validates our work but acts as the fuel that keeps our team moving forward every day.